
Transtheoretical Model: The Definitive Guide
Last updated: March 2026
Transtheoretical Model
The Definitive Guide
Have you noticed that some people are far more willing or ready to change their behavior as compared to others?
Scientific models such as the Transtheoretical Model can help us understand the detailed process of ‘change’ that one goes through.
So if you want to:
- Learn about the fundamentals of the Transtheoretical Model.
- Discuss the six stages of change.
- Find out the most common outcomes of the Transtheoretical Model.
- Learn how you can incorporate the model into your practice to benefit your clients.
This article should help you understand the mental process that one goes through before making a decision, which will be of real value to you.
So let’s get started!!
Contents
Chapter 1
The Fundamentals
Chapter 2
Discussing the six stages of change in detail
Chapter 3
Decisional Balance of Change and Self Efficacy for Change
Chapter 4
Outcomes of The Transtheoretical Model
Chapter 5
Critiques of the Transtheoretical model
Chapter 1:
The Fundamentals
This chapter will focus on the basics of what you need to know about The Transtheoretical Model (TTM).
I will walk you through what exactly the model means, what it deals with, and the history of the model. Lastly, I will give a brief introduction to the six stages of change according to the model.
Let’s begin!
What is The Transtheoretical Model (TTM)?
The Transtheoretical Model (aka TTM) is a theoretical model of behavior change which helps one assess the willingness of an individual to adapt to new and healthier behaviors.
The assessment also provides a guideline full of processes and strategies to help the individual achieve the desired “healthy” behavioral outcome.
TTM is touted to be one of the best models to bring positive behavioral change by many self-help books such as Changing for Good (1994), Changeology (2012), and Changing to Thrive (2016).
It has also been quoted several times in various news articles.
It has been called "arguably the dominant model of health behavior change, having received unprecedented research attention” by Christopher Armitage in the British Journal of Health Psychology.
What does the Transtheoretical Model deal with?
TTM mainly focuses on change, and breaks it down into the sub-stages which an individual goes through while making any change to their behavior.
Each stage is then further elaborated upon, and identifying characteristics of the stage are clearly defined.
The model then goes a step further to give tools of guidance to people who are helping the individual bringing change (aka coaches, therapists, etc.), for each step of the change.
In short, the model has taken the intangible concept of change and broken it down scientifically, to not only understand the process, but also to manipulate it for the behavioral betterment of people.
The model even helps get rid of people’s aversion to change by providing easy navigational steps to bring about change easily.
History of the Transtheoretical Model
Beginning in the late 1970s, the Transtheoretical Model was created by James O. Prochaska from the University of Rhode Island, Carlo Di Clemente, and colleagues. It is based on the analysis and application of many psychotherapy theories, hence the term ‘transtheoretical’.
They were trying to understand why some people find it easy to quit smoking on their own, while some people needed therapy and extensive methods of surveillance and checks to successfully quit smoking.
Eventually, on the basis of studies published in peer-reviewed publications and books, Prochaska and his colleagues refined the model.
Consequently, the TTM focuses on individual decision-making and is a model of deliberate transformation.
The TTM is based on the premise that people do not alter their behavior fast or decisively.
Rather, change in behavior, particularly habitual behavior, is a cyclical process that occurs continuously.
The TTM is a model, not a theory, and other behavioral theories and constructs can be applied to different stages of the model depending on their effectiveness.
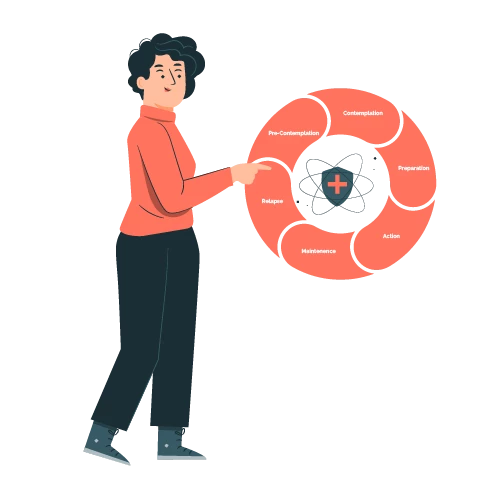
Introduction to the Six Stages of Change
According to the TTM, there are six basic stages of change that a person goes through. As mentioned before, the model is not linear, but, rather, cyclical.
So, a person can go through these stages like a cycle in order to achieve the desired results.
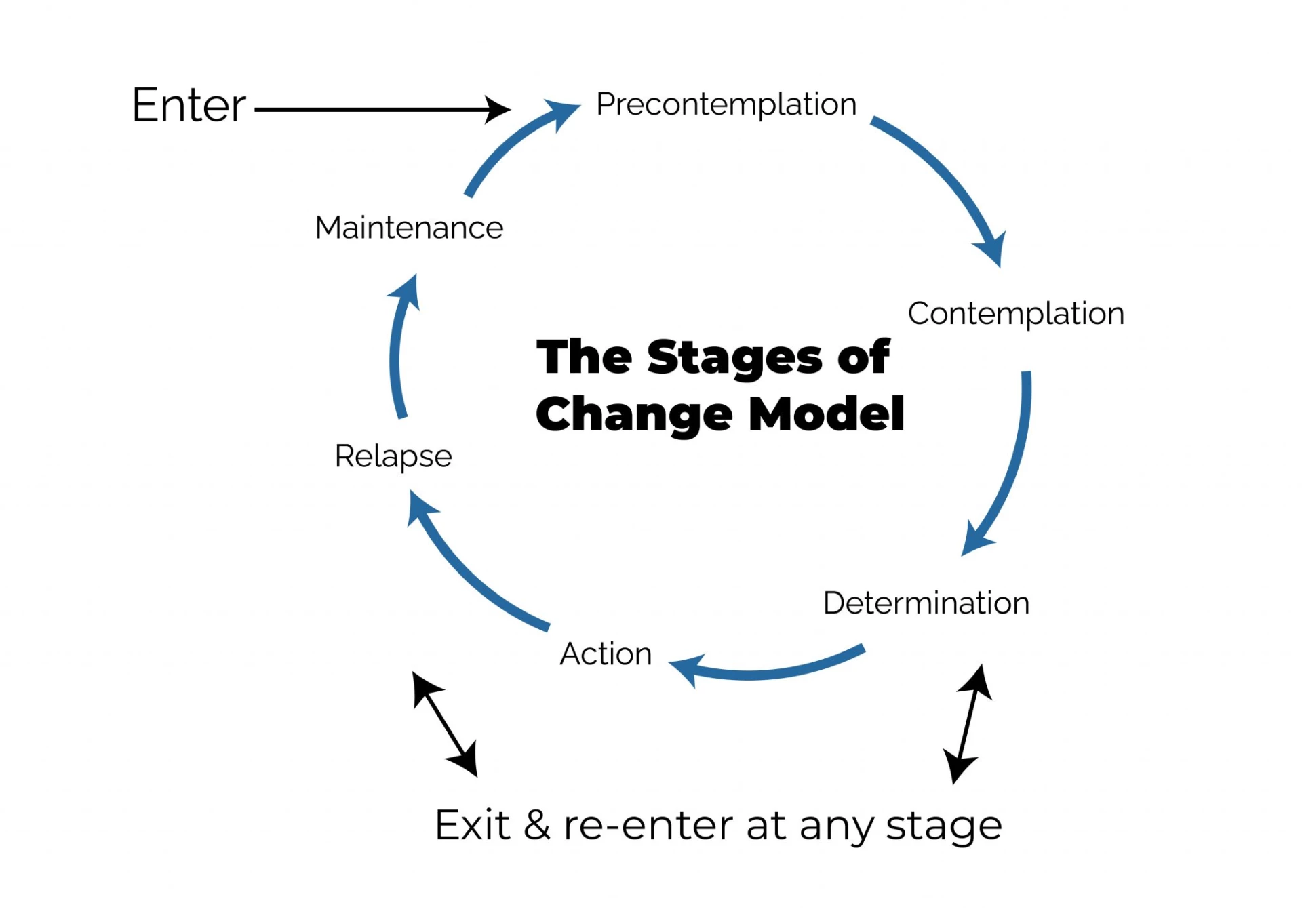
Thus, the six main stages of change as per the TTM are:
- Precontemplation
At this point, people have no plans to act in the near future (defined as within the next 6 months).
People are frequently ignorant that their actions are harmful or have negative consequences.
People at this stage frequently undervalue the benefits of changing their behavior, and place far too much focus on the disadvantages.
- Contemplation
During this stage, people are considering starting a good habit in the near future (defined as within the next 6 months).
People notice that their conduct may be harmful, and they analyze the benefits and drawbacks of modifying their behavior more carefully and practically, with equal weight given to each.
Even after recognising this, people may still be hesitant to change their habits.
- Preparation (Determination)
At this level, people are ready to act in the next 30 days.
People begin to change their behavior in modest increments, believing that changing their conduct would lead to a healthier existence.
- Action
People in this stage have recently modified their behavior (defined as within the last 6 months) and aim to keep that behavior change going.
This can be demonstrated by people changing their troublesome behaviors, or learning new, healthy ones.
- Maintenance
People at this stage have maintained their behavior change for a long time (defined as more than 6 months) and aim to keep it going in the future.
They also work hard to avoid relapsing to a previous stage.
- Termination
People who have reached this stage have no desire to return to their unhealthy behaviors, and are confident that they will not relapse.
This stage is typically overlooked in health promotion initiatives since it is rarely achieved, and people tend to stay in the maintenance stage.
Now that we know the six basic stages of change according to the TTM, I am going to expand upon each stage in the next chapter. I will also share tips to succeed in each stage of the TTM, according to the model itself.
Chapter 2:
Discussing the six stages of change in detail
In this chapter, I will categorically expand upon the six stages of change mentioned above.
The chapter will also have some actionable tips that one can use in each stage of change to achieve desirable results, and to move to the next step successfully, without having to get stuck. Coaches can use these tips to guide their clients towards their results.
Stage 1: Precontemplation (not ready)
People at this stage are unlikely to modify their habits in the near future (within six months) and may be uninformed of the need to do so.
People learn more about healthy conduct here: they are encouraged to consider the benefits of changing their behavior, and to express their feelings about how their negative behavior affects others.
Precontemplators frequently undervalue the benefits of change while exaggerating the drawbacks, and they are often unaware that they are doing so.
What can a coach do during this stage?
Coaches can encourage them to become more careful of their decision-making.
Coaches can also make them aware of the numerous benefits of quitting unhealthy behavior. These will be the two most effective actions that coaches can take to assist their clients at this point.
Stage 2: Contemplation (getting ready)
In this stage, clients aim to begin healthy behavior within the following six months.
While they are usually more aware of the benefits of switching to more positive behavior, the disadvantages of this “change” are roughly equivalent to its advantages.
Because of their apprehension about change, clients may continue to put off taking action.
In this stage, people also learn about the kind of person they could be if they adjusted their conduct and learn more from healthy people.
What can a coach do during this stage?
Coaches can effectively influence and assist individuals at this stage by urging them to work on minimizing the disadvantages of changing their habits.
Also, they can help clients visualize their better future as a result of the desired behavioral change.
Remember – in this stage, people are still unsure of the need to change their behavior. So, you, as a coach, need to convince them that the step they are about to take is important.
Visualization of the future is key here.
Stage 3: Preparation (ready)
At this point, people are ready to take action within the following 30 days.
They take modest measures that they feel will help them incorporate healthy habits into their daily life. They inform their friends and family, for example, that they desire to modify their ways.
What can a coach do during this stage?
Clients at this stage should be encouraged to seek help from trusted friends, tell others about their plans to modify their behavior, and consider how they would feel if they behaved in a better manner.
Their main anxiety is that if they act, they will fail. They discover that the better prepared they are, the more likely they are to continue to advance.
And your job as a coach is to help them calm this anxiety by encouraging them to speak more about their desired change and again, visualize the better life that will be created as a result of this change.
Stage 4: Action (current action)
People at this stage have changed their behavior in the last six months and must work hard to maintain their progress.
These individuals must learn how to deepen their commitments to change, and resist the impulse to revert.
What can a coach do during this stage?
Coaches in this stage can help their clients learn techniques for sticking to their commitments.
Some of these would include substituting positive activities for activities associated with unhealthy behavior, rewarding themselves for taking steps toward change, and avoiding people and situations that tempt them to behave in unhealthy ways.
Coaches can also use models such as the GROW model to help clients set achievable goals and stick to them. I have expanded in detail how one can use the GROW model of goal setting in this article.
Stage 5: Maintenance (monitoring)
People in this stage have adjusted their behavior for at least six months.
It's critical for people at this stage to be mindful of situations that can entice them to revert to their old habits, especially stressful situations.
What can a coach do during this stage?
Coaches need to encourage clients in this stage to seek assistance from, and chat with, individuals they trust.
Clients should also be encouraged to spend time with people who behave in healthy ways, and remember to cope with stress through healthy activities (such as exercise and deep relaxation), rather than their unhealthy behavior.
Another important and extremely common step during maintenance is ‘relapse’.
Relapse in the TTM is specifically for those clients who have successfully quit smoking, using drugs, or drinking alcohol, or any other hazardous habits only to return to them.
People who try to quit highly addictive activities like drug, alcohol, or nicotine usage are especially vulnerable to relapse.
Long-term behavior change frequently involves continual support from family members, a health coach, a physician, or another source of encouragement. Supportive literature and other resources can also be beneficial in preventing a recurrence.
Stage 6: Terminance
People at this stage have no desire to revert to their bad habits and are confident that they will not relapse.
This stage is typically overlooked in health promotion initiatives, since it is rarely achieved and people tend to stay in the maintenance stage.
Mental Steps that Comprise the Processes of Change
The 10 processes of change include ‘covert and overt activities that people employ to proceed through the stages’.
People use cognitive, emotive, and evaluative processes to progress through the early stages. People rely more on commitments, counter conditioning, rewards, environmental restrictions, and assistance as they proceed toward Action and Maintenance.

According to Prochaska and colleagues' research on the Transtheoretical Model, interventions to alter behavior are more effective if they are ‘stage-matched’ or ‘suited to each individual's stage of change.’
People, in general, require the following in order to progress:
- Decisional Balance
The TTM refers to this as an increasing knowledge that the benefits (the "pros") of changing exceed the difficulties (the "cons"). We will look at this deeper in the next chapter.
- Self-efficacy
Self-efficacy, according to the TTM, is the belief that individuals can make and maintain their changes in situations that entice them to return to their old, harmful behavior.
We will assess this in depth in the next chapter.
- Processes of change
The TTM refers to the processes of change as strategies that can assist clients in making and maintaining the change made.
Let’s take a deeper look into the processes of change as they help clients maintain their change.
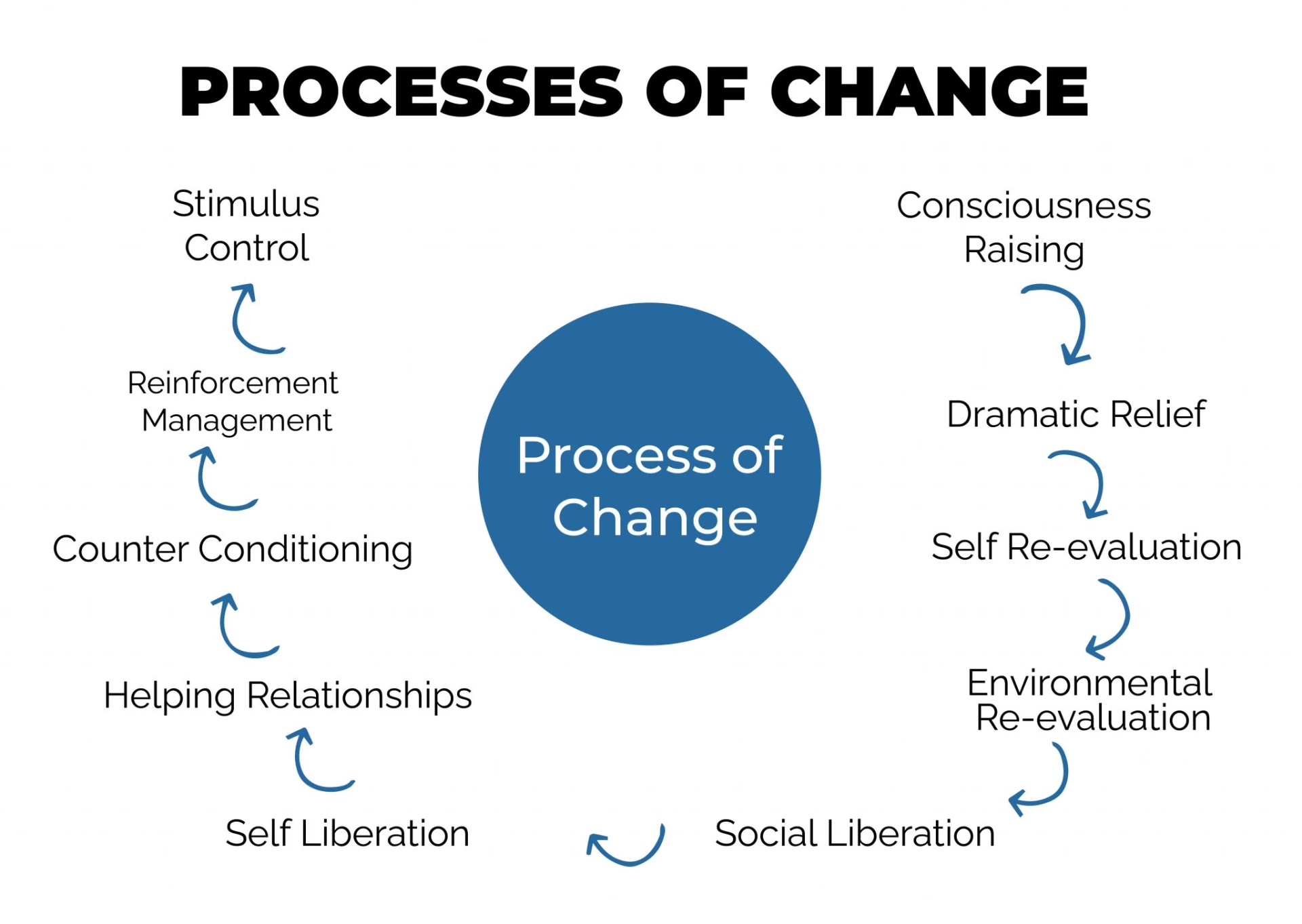
- Consciousness-raising
Improving awareness of good behavior through information, education, and personal feedback.
- Dramatic relief (or paying attention to feelings)
Paying more attention to fear, anxiety, or worry which came as a result of the harmful behavior, or inspiration and hope which arrived as a result of hearing about how others have been able to convert to healthier habits.
- Self-reevaluation (or creating a new self-image)
Self-reevaluation (creation of a new self-image) — acceptance that healthy behavior is an important aspect of who they wish to be.
- Environmental reevaluation (or noticing your effect on others)
Environmental reevaluation indicates seeing how someone’s bad behavior affects others, and how they might change to have a more positive impact.
- Social liberation (or noticing public support)
Discovering that society encourages healthy behavior.
- Self-liberation (or making a commitment)
Believing in one's potential to change, and making commitments and re-commitments to follow through on that belief.
- Helping relationships (or getting support)
Finding individuals who are encouraging of the shift they are aiming for in their lives.
- Counterconditioning (or using substitutes)
Substituting unhealthy habits of behavior with better and healthier ways.
- Reinforcement Management (or using rewards)
Boosting incentives for positive behavior, while decreasing rewards for negative behavior.
- Stimulus Control (or managing your environment)
Employing reminders and cues that encourage healthy behavior while avoiding those that do not.
The first five processes of change are based on cognitive and affective experiential processes. They focus on the internal dialogue that happens in the head of any individual.
During these five processes, the individual has to really focus on maintaining a healthy internal dialogue.
The last five processes, however, focus more on the behavioral aspects of an individual’s path to change.
These can easily be controlled and observed by well-wishers, coaches, therapists, etc.
As a coach, you will have to be there to reinforce good and healthy thoughts during the first five stages, while motivating clients to show their positive changes in the last five processes.
Now that we know in depth the processes of change, I will expand upon the other two parts of the TTM which go hand-in-hand with the stages of change – self-efficacy and decisional balance, in the next chapter.
I will also discuss their importance, and ways to identify these stages.
Chapter 3:
Decisional Balance of Change and Self Efficacy for Change
The six stages of the TTM are the crux of the model but it is incomplete without the full understanding of decisional balance and self-efficacy.
These two concepts are what motivates an individual to go successfully through all the six stages of the TTM.
In this chapter, I will delve into both of them in depth, and discuss why they are so important.
What is decisional balance, and what is its relevance to the TTM?
This key construct reflects the individual's relative weighing of the benefits and drawbacks of change.
Janis and Mann (1977) defined decision-making as a ‘decisional balance sheet,’ containing relative potential rewards and costs.
The advantages and disadvantages of decisional balance measures have become essential components in the Transtheoretical approach.
The advantages and disadvantages combine to create a decisional ‘balance sheet’ of prospective benefits and losses. Depending on which stage of transformation an individual is in, the positives and negatives are weighted differently.
- When a person is in the Precontemplation stage, the benefits of changing one's conduct are overshadowed by the disadvantages of changing one's behavior and the benefits of preserving one's current behavior.
- The positives and drawbacks tend to have equal weight in the Contemplation stage, leaving the individual uncertain about change.
- Many people progress to the Preparation, or even the Action stage, if the decisional balance is skewed in their favor, that is – the benefits of changing outweigh the disadvantages of continuing the unhealthy behavior.
- In order to reduce the likelihood of relapse, the benefits of keeping the behavior change should balance the disadvantages of maintaining the change as individuals enter the Maintenance stage.
Taking all of this into consideration, the following correlations are seen between the benefits, drawbacks, and stage of change have been discovered by TTM study spanning 48 behaviors and 100 populations.
- The disadvantages of changing outweigh the advantages in the Precontemplation stage.
- The advantages surpass the disadvantages in the middle stages.
- The advantages outweigh the disadvantages in the Action stage.
Self-efficacy According to the TTM, and Its Importance
Bandura's Self-efficacy Theory is incorporated into the TTM (Bandura, 1977, 1982).
This construct indicates how confident people are in their ability to maintain their desired behavior change under settings that frequently lead to relapse.
It's also determined by how tempted people are to return to their problematic behavior in high-risk scenarios.
Temptation to engage in the problem activity is significantly larger than self-efficacy to abstain, during the Precontemplation and Contemplation stages.
The gap between sentiments of self-efficacy and temptation diminishes as people progress from Preparation to Action, and behavior change is achieved.
Relapse is common in instances where people's feelings of temptation outweigh their sense of self-efficacy to keep the desired behavior change.
In short, self-efficacy or the ability to control temptations and urges to give in to negative behavior is highly important to maintain successful progression through all the stages of change.
Some people generally tend to have better self-efficacy than others.
However, self-efficacy can be improved by coaches by keeping clients accountable for their actions and fostering better communication pathways with clients.
All of these steps will help you understand how to navigate efficiently through stages of change with your clients. But you will also need to understand and be realistic about the outcomes you may see your client achieving.
I have expanded upon these outcomes in the next chapter.
Chapter 4:
Outcomes of The Transtheoretical Model
Now that we have seen all the important stages of changes and other things needed to make successful behavioral changes, we need to focus on the outcomes usually seen as a result of the Transtheoretical Model.
The TTM was researched on people trying to quit smoking and, eventually, on people trying to have better health-related behavior, so a lot of these outcomes are health related.
However, there can be parallels drawn even to other aspects of life and other outcomes.
Where is the Transtheoretical Model used most often, and for which kind of outcomes?
Like I mentioned earlier, the TTM is most often used to assess outcomes related to smoking management, specifically, cessation of smoking.
But some other uses of the TTM are related to stress management, understanding behavior linked to modes of transportation, weight management, depression management, etc.
Common TTM outcomes
Let’s look at some of the most common TTM outcomes that I mentioned above.
- Cessation of Smoking
According to the original research by Prochaska and colleagues, people who wanted to quit smoking who took help of the TTM, were more likely to not relapse into smoking as compared to other people who did not make use of the TTM.
TTM was combined with other methods such as best-in-class action-oriented self-help programs, non-interactive manual-based programs, and other common interventions.
- Stress Management
A stress management intervention was given to a group of pre-Action individuals in the United States.
When compared to the control group, a considerably higher proportion of the treatment group (62%) was successfully managing their stress at the 18-month follow-up.
The intervention also resulted in statistically significant reductions in stress and depression, as well as an increase in the usage of stress management techniques.
Prochaska et al. and Jordan et al. observed considerably higher proportions of treatment groups effectively managing stress as compared to control groups in two further clinical studies using TTM programmes.
- Understanding Behavior Linked to Modes of Transportation
Another innovative study assessed people’s willingness to switch to more sustainable ways of transportation such as biking/walking.
The motivators identified are liking to bike/walk, avoiding congestion, and improved fitness.
Perceived barriers are personal fitness, time, and the weather. This knowledge was used to design interventions that would address attitudes and misconceptions to encourage an increased use of bikes and walking.
The researchers have a hypothesis that combining sustainable traveling with health benefits will lead to better chances of experiencing changed behavior.
- Weight Management
In a 2014 comprehensive review, the effectiveness of using this model in weight management therapies for overweight and obese people (containing food or physical activity programmes, or both, and especially when combined with additional interventions) was investigated.
The findings revealed that there is inconclusive evidence about the impact of these therapies on long-term weight loss (one year or longer).
Based on relatively moderate scientific evidence, this technique may create good impacts on physical activity and eating behaviors, such as increased exercise duration and frequency, fruits and vegetable consumption, and dietary fat intake reduction.
- Depression Management
350 primary care patients who were depressed, but not in treatment or planning to seek treatment for depression in the next 30 days, were included in the study.
During the 9-month follow-up period, patients who received the TTM intervention had considerably more symptom reduction. Patients with moderate to severe depression who were in the Precontemplation or Contemplation stage of change at baseline saw the greatest benefits from the intervention.
For example, rates of reliable and clinically significant improvement in depression were 40% for treatment, and 9% for control, among patients in the Precontemplation or Contemplation stages.
During the follow-up period, the intervention helped patients with mild depression or who were in the Action or Maintenance stage at baseline prevent disease progression to Major Depression.
Of course, apart from these uses, there can be a lot more uses of the TTM. Any time an individual is trying to change their habits, at least a part of – if not the whole TTM – can be used successfully as a tool.
However, no good theory will be complete without critiques. So, the next chapterwill focus on understanding some of the most common critiques of the model.
Chapter 5:
Critiques of the Transtheoretical model
The Transtheoretical Model is basically just a scientific theory, and no theory is complete without critiques.
Critiques help researchers better their understanding of any topic and strive hard to make models near perfect.
What are some common critiques of the TTM?
Let’s take a closer look at some of the most commonly found critiques of the model that one must be cognizant about while using the TTM as a tool.
- The hypothesis overlooks the social context in which change takes place, such as socioeconomic standing and income.
- There are no standard criteria for determining a person's stage of transition, hence the borders between the stages can be arbitrary.
- The surveys used to categorize people into stages of transition are not always uniform or validated.
- There is no clear understanding of how much time each stage requires or how long a person can stay in a stage.
- When it comes to decision-making, the model implies that people develop coherent and rational plans, which isn't always the case.
So we, as coaches, need to make sure we take the TTM with a pinch of salt.
With that being said, it is important to understand that the TTM is still a very valid and helpful tool to understand the stages of change and help clients navigate them successfully.
Conclusion
Congratulations on making through this article and learning a new and important model linked to behavioral change!
Now that you know this, you can be more aware of the different stages related to change that one goes through and how you as a coach can help one switch to healthier habits. You can also use this model to self-assess your method of bringing changes in your life.
Have you incorporated this model into your practice yet?
Which stage of change did you find most challenging to take your client to?
What have been your biggest learnings from this process?
Let us know in the comments below!
